Learn the Internal fixation of proximal forearm fracture: Henry’s approach to the forearm surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Internal fixation of proximal forearm fracture: Henry’s approach to the forearm surgical procedure.
Henry’s approach was first described in 1945 by Arnold K Henry, Emeritus Professor of Surgery at the University of Egypt and a fellow of the Royal College of Surgeons of Ireland. His book, “Extensile Exposure applied to limb surgery” is a landmark publication in Orthopaedic education and a work of time-proven genius.
Now, 79 years after it published if you could get hold of a copy the clarity of its text and its few perfectly executed drawings would by themselves still guide a half decent surgeon safely through a number of key areas for the first time.
The best in my opinion are his exposures to the posterior thigh and calf, the posterior humerus and to the volar aspect to the forearm, which it is my pleasure to demonstrate in this technique.
Henrys’ original landmarks were proximally the biceps tendon insertion into the proximal radius (radial / lateral side); to the distal radius styloid. Subsequently it has been modified so that distally the landmark is the Flexor Carpi Radialis (FCR) tendon / volar scaphoid tubercle. Surgeons will be familiar with the FCR approach for the fixation of distal radius fractures and access to the distal third of the radius, this is sometimes called the Modified Henry’s approach.
The approach utilises an internervous plane:
- Proximally between brachioradialis (radial nerve) and pronator teres (median nerve).
- Distally between brachioradialis (radial nerve) and flexor carpi radialis (median nerve).
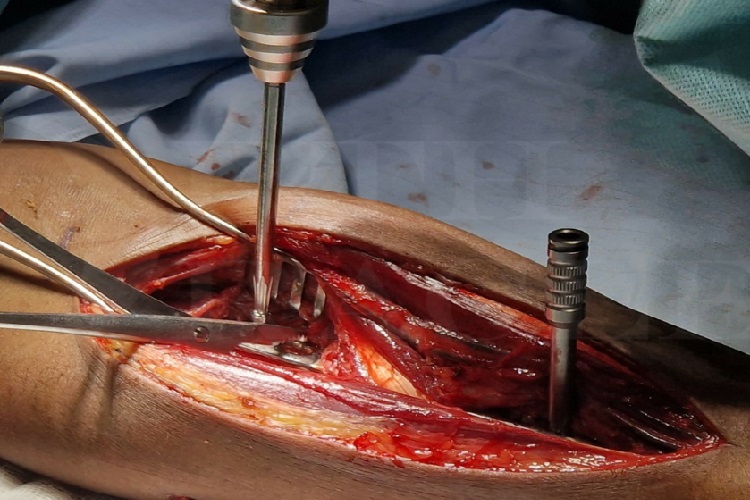
Although it uses an internervous plane between the muscles, the actual approach at the superficial level is between the radial artery and superficial radial nerve, and both must be carefully dissected and protected throughout the procedure. I recommend that the nerve and vessel are inspected at the end of the procedure to ensure their continuity and assuage any concerns that you may experience in the follow up clinic, if there is any superficial radial nerve dysfunction.
In this case I’ve used the approach for access to a very comminuted fracture of the proximal and middle third of the radius caused by a gunshot injury. This is a challenging case as the comminution makes it difficult to correctly judge the true radial length, alignment and rotation. Also the pronator teres insertion can act as a deforming force displacing the reduction or obstructing access to the radius, and may need to be released. The following technique will describe strategies for how to address each of these challenges.
OrthOracle readers will find the following associated instructional techniques also of interest:
Galeazzi radial fracture-dislocation: Fixation using Synthes LCP locking plate
Open Reduction Internal Fixation of a Monteggia forearm fracture dislocation using the Synthes small fragment LCP plate
Ulnar corrective osteotomy: Distal periarticular osteotomy fixed with Synthes Hook plate
Author: Mr Ross Fawdington FRCS (Tr & Orth)
Institution: The Queen Elizabeth hospital, Birmingham, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu